
Woah, hopefully the title was an attention-grabber, but there’s a purpose to this.
In medical training, hopefully along the line, we all have the discussion about something called “Cultural Competence,” which is defined by the American Psychological Association as: The ability to understand, appreciate and interact with people from cultures or belief systems different from one’s own. Generally, people in Medicine most commonly refer to this in taking care of someone of a different religious, ethnic or social background than their own – as examples, things like respecting traditions and preferences for a human that is Latino or a Jehovah’s Witness or Homeless or anything else that isn’t what we are. But, the things we don’t talk about as often are cultural differences within the medical community itself. Traveling from one state to the next, one practice to another, I have seen medical practices vary in accordance sometimes with the surrounding demographic, but also based on the experience and background of the providers. I’m not saying that one answer is better than another, but it’s fascinating to see how the Doctors in one area practice differently than another, based on how they were maybe “raised”; especially when there are not extremely clear guidelines from overarching medical societies or academies.
There are tons of examples of this but the biggest two which are always at the forefront of discussions in MY world are: Circumcisions and Frenotomies (a.k.a. tongue tie clipping).
CIRCUMCISIONS. Disclaimer: This is NOT a post to talk about the controversy over recommendations for circumcisions – for the record, per the AAP, I have no professional recommendation and follow cultural/familial preferences, do whatever you want. Many people are surprised when I tell them that most Pediatricians do NOT perform Circumcisions. I’m sure there’s some sort of actual history to this, i’m too lazy to actually look into it for this post, eventually we’ll do that… But, in regards to the medical providers that CAN do the actual procedure for newborns specifically, this is generally an OBGYN, a Pediatrician, a Family Medicine doctor, or if you’re lucky a Urologist (penis specialist) – I know some nurse practitioners and physician’s assistants that also routinely perform them. According to some random 1997 Article I Googled, at that time per a survey only 35% of Pediatricians did Newborn Circumcisions; who knows if that’s true… But, I can say that among 100 Pediatric residents that I trained with, I know of only ONE other that sought out Circumcision training as I did; it was surely not routinely taught to us. Lucky for me, my tutelage was from a great Pediatric Urologist in Texas and further with an OBGYN from the West Coast, so, I do feel as if I personally had great and reliable training.
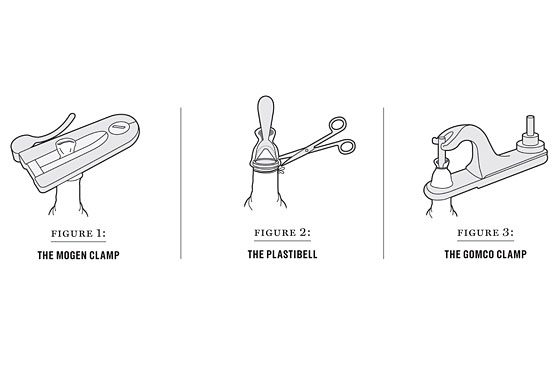
That being said, regardless of whoever does it, there are THREE different methods for the procedure: The Gomco Clamp, The Plastibell Device, and The Mogen Clamp. I myself perform the Gomco Clamp – the same technique performed by my mentors, who combined do more than >150 procedures per month. After traveling to multiple campuses across the country, the general trend is that many OBGYNs perform Mogens and most Pediatricians perform Gomcos and rarely Plastibells. Studies have compared these various techniques and in the end, as long as the operator is skilled and careful, there is really no long term difference; the rates of complications seem to be similar. So, I found it fascinating when I showed up for my first day at a new facility and found out that not only is the culture here to perform the Mogen Clamp, but that many of the Pediatricians have actually CONVERTED from the Gomco TO the Mogen 😮. I can see the pros and cons for both, but it was my first facility where this was the preferred technique even amongst my peers. Will I change my practice now that I’ve come across a variation in something I thought I knew well? Would I really be learning or growing if I didn’t at least consider it?

FRENOTOMIES. “Tongue tie clipping” has become more and more common in the United States. This is a HUGELY controversial topic and I’m not really here to argue about it… But I WILL leave this here: Why So Many Babies Are Getting Their Tongues Clipped (The Atlantic, 2019). Personally, I feel it is driven by specific medical professionals, but the evidence for its necessity long term in babies that don’t have difficulty with feeding, is very lacking. However, with good reason and physiologic understanding, I can simultaneously understand how it could cause a real problem and how performing the procedure could make a tangible difference. Basically, a “tongue tie” is when the tongue is attached underneath to the gum/gingiva in a way that restricts movement. If you can’t raise your tongue to the roof of your mouth it makes it harder to eat and in theory to speak down the line; so, a procedure to cut that little thready attachment called a “Frenotomy” can be performed with a little knife or with a laser. Where I trained in Texas, it was unanimously NOT done – none of the ENT or Plastic Surgeons I worked with (holding a cumulative 50+ years of experience) would perform it at one of the largest academic institutions in the United States. Oddly, with my travels, I have now come across a few institutions where it is HIGHLY performed. Even within those institutions I have come across a few where the PHYSICIANS are highly against it while the APPs (Advanced Practice Providers or Mid-Level Providers) are the only ones that perform it and another where the General Pediatricians do it themselves. So, it creates a whole lot of questions and thoughts. I was raised to be very against this minor procedure; but, as I come across more and more providers that do this procedure my world has been opening up to the utility of it. I definitely don’t plan on ever performing the procedure myself, but maybe i’ll be more open-minded to the benefits and outcomes, despite my continued personal disbeliefs.
There is always more than one way to skin a… Deer. If two different doors lead to the same outcome, does it matter which one you took? Every day I come across variations in practice that expand my tools, mindset and availability to receive new information. The more I discover new medical culture, the more I’m able to develop an amalgamation of various information into the best combination of everything. Ultimately, these little glimpses of culture shock are infinitesimally appreciated into me becoming the Best Doctor I can be. I still love locum tenens.
